The Federal Floor Just Moved Down. Everyone Else Is Moving Up.
This week the regulatory map redrew itself, and in opposite directions in adjacent agencies. HHS proposed rolling back AI health IT transparency requirements that have been the floor for vendor accountability since 2024. The FDA cleared the first continuous AI sepsis monitoring system with an 18% mortality reduction endpoint. MACPAC formally recommended that CMS tighten oversight on AI used in Medicaid prior authorization. Three federal moves, three different directions, one structural signal: the era of a single coherent federal posture on healthcare AI is ending. The systems that already operate in production extended their lead. The systems still scoping pilots are about to find that the map has been redrawn around them.
1. Signal Summary
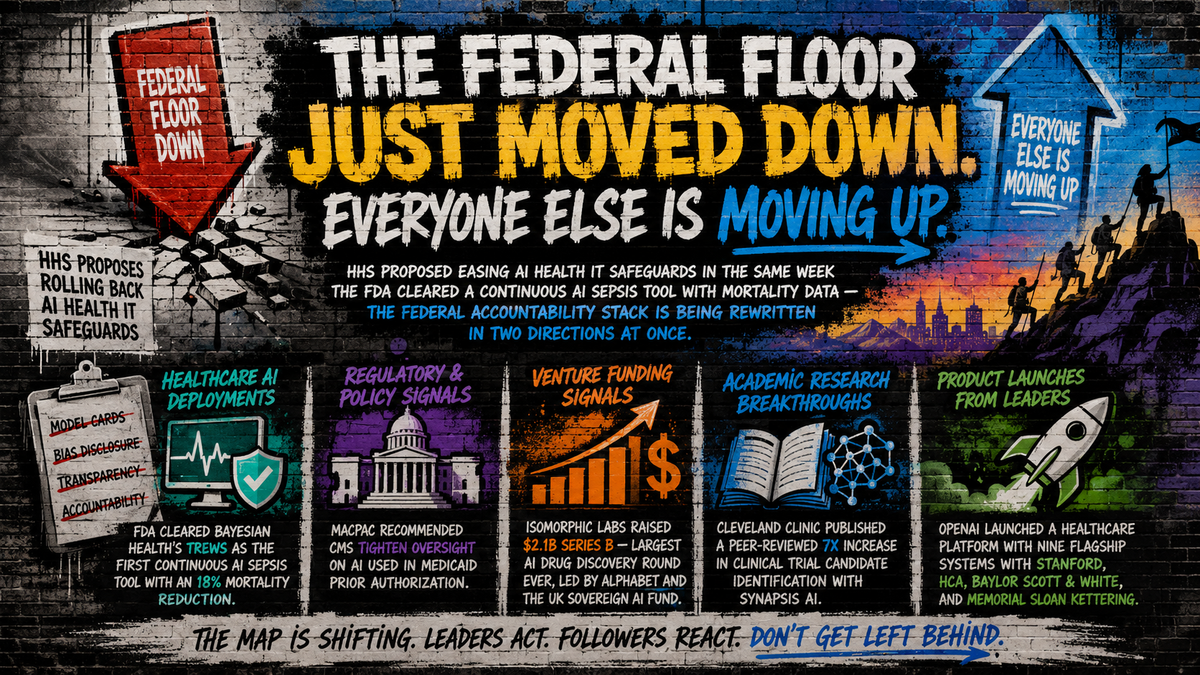
- HHS proposed easing AI health IT safeguards. Trump/Kennedy rulemaking targets model card and bias disclosure requirements; AHA, ACP, Altera, and Abridge push back publicly.
- FDA cleared Bayesian Health's TREWS as the first continuous AI sepsis tool, with an 18% mortality reduction across multi-site validation at Cleveland Clinic, MemorialCare, and University of Rochester.
- Cleveland Clinic published a peer-reviewed 7x increase in clinical trial candidate identification with Synapsis AI.
- MACPAC formally pushed CMS to tighten transparency and human-oversight requirements on AI in Medicaid prior authorization.
- Isomorphic Labs raised $2.1B Series B, the largest AI drug discovery round ever, led by Alphabet and the UK Sovereign AI Fund.
- OpenAI launched a healthcare platform with nine flagship systems including Stanford, HCA, Baylor Scott & White, and Memorial Sloan Kettering.
2. Big Signal of the Week
HHS Proposes Easing AI Health IT Safeguards. The Vendor Accountability Floor Is Now Negotiable.
🔴 Policy / Regulation | Score: 8.5 (High Signal) | View Article
Why It Matters A Trump/Kennedy HHS proposal would roll back AI health IT transparency provisions, including model card and bias disclosure requirements, that have functioned as the floor for vendor accountability since the 2024 HTI-1 rules. AHA, ACP, and named EHR and ambient AI vendors (Altera, Abridge) pushed back publicly within hours. The proposal would not eliminate vendor liability. It would redistribute it to payer audits, state laws, and tort exposure already moving in the opposite direction.
Key Details
- Source: HHS proposed rulemaking, mid-May 2026
- Provisions targeted: Model card requirements, bias disclosure mandates, transparency to clinicians and patients
- Named pushback: American Hospital Association, American College of Physicians, Altera Digital Health, Abridge
- Companion regulators moving the opposite direction: FDA (Bayesian sepsis clearance with mortality endpoint), MACPAC (Medicaid prior auth oversight), state AGs (Pennsylvania v. Character.AI, ongoing)
What This Signals Federal compliance is becoming a less reliable signal of what good AI governance looks like. The vendors most exposed are the ones who built their compliance posture exclusively against the HTI-1 floor.
My Read The AHA-plus-Abridge pushback coalition is doing the political work most coverage missed. When the hospital lobby and ambient AI vendor lobby are on the same side of a comment letter, the proposal has united two groups that expected to benefit from rollback on different timelines. Looser federal rules do not reduce vendor accountability. They redistribute it to harder venues: state AGs, payer audit programs, and tort exposure. The actionable move this quarter: assume the federal floor is moving down, assume state and payer floors are moving up, and rebuild AI vendor procurement against the higher of the two. Add contractual clauses requiring continued HTI-1-level transparency posture regardless of HHS rulemaking. Vendors that resist are telling you something about their actual capability.
Source: Fierce Healthcare
3. Real World Deployments
Cleveland Clinic + Synapsis AI: 7x Lift in Trial Candidate Identification (Peer-Reviewed)
🔴 Real-World Deployment | Score: 8.5 (High Signal) | View Article
Why It Matters Cleveland Clinic, working with Synapsis AI, documented a seven-fold increase in eligible candidate identification for a Phase III polycythemia vera trial. The peer-reviewed study reports 100% positive predictive value on reviewed picks, candidate identification in days versus months of manual chart review, and reduced research coordinator screening time.
Key Details
- Organizations: Cleveland Clinic, Synapsis AI
- Use case: Phase III oncology trial recruitment (polycythemia vera)
- Outcome: 7x increase in eligible candidate identification
- PPV: 100% on reviewed AI-identified candidates
- Time-to-screen: Days vs. months of manual chart review
- Publication: The ASCO Post (peer-reviewed)
What This Signals Trial recruitment is the highest-friction, lowest-yield operational task in academic medicine. A peer-reviewed 7x lift resets the procurement bar for every academic medical center competing for industry-sponsored trials.
My Read Industry trial sponsors will quietly favor sites with documented recruitment velocity in the next RFP cycle. Any academic medical center without an active LLM trial matching evaluation is now visibly behind a flagship competitor with peer-reviewed evidence. The strategic question is no longer whether to deploy. It is whether your IRB workflow, EHR data export pipeline, and screening governance survive a pharma sponsor due-diligence question they were not being asked 90 days ago.
Source: The ASCO Post
Stanford Healthcare Hits 60% Utilization on Enterprise Admin AI
🔴 Real-World Deployment | Score: 8.2 | View Article
Why It Matters Stanford Healthcare deployed AI enterprise-wide to automate billing inquiry responses, draft test results, and accelerate software development, reporting 60% utilization across deployed workflows. The deployment is administrative, not clinical decision support, which is exactly where Stanford is booking measurable near-term ROI.
Key Details
- Organization: Stanford Healthcare
- Use cases: Billing inquiry automation, test result drafting, software development acceleration
- Achieved metric: 60% utilization across deployed workflows
- Deployment scope: Enterprise-wide
- ROI category: High-volume, low-complexity administrative tasks
What This Signals Administrative AI, not clinical decision support, is the cleanest 2026 ROI line. Capital planners should treat Stanford's portfolio mix as a forward indicator: 12 months of admin AI ROI funds the next 24 months of clinical AI investment.
My Read The 60% utilization number is the one that matters operationally. Deployment is not adoption, and most enterprise AI announcements quietly trail off when measured by actual usage. Stanford publishing a 60% number is a credibility move that creates a procurement benchmark every comparable admin AI vendor now has to answer to. CIOs running multi-vendor admin AI portfolios should add utilization-rate disclosure to vendor reporting requirements this quarter.
Source: CIO Magazine
Sentara Health: 70,000 Virtual Nursing Encounters with Improved Patient Ratings and Time Savings
🔴 Real-World Deployment | Score: 7.6 | View Article
Why It Matters Sentara Health rolled out virtual nursing across its hospitals integrated with ambient AI documentation, reporting over 70,000 encounters with improved patient ratings and early time savings on admissions and discharges. Distinct from the UCHealth virtual ICU deployment covered in Issue 7 (April 28); Sentara's is acute care, system-wide, with achieved metrics.
Key Details
- Organization: Sentara Health
- Use case: Virtual nursing with ambient AI documentation
- Volume: >70,000 encounters documented
- Patient experience: Improved patient ratings
- Workforce outcome: Early time savings on admissions/discharges
- Deployment scope: System-wide acute care
What This Signals Virtual nursing now has multi-system production validation across UCHealth (Issue 7), Abridge nursing GA at 250+ systems (Issue 9), and Sentara, with documented patient experience and workforce metrics. The staffing crisis is the deployment forcing function. The procurement template is becoming standardized.
My Read The patient ratings improvement is the underrated detail. Virtual nursing models typically lose patient-experience points relative to bedside-only care; Sentara reversed that signal, which makes the labor-substitution case defensible to CNOs and patient experience officers in the same conversation. The remaining strategic question is what the recovered nursing time funds (patient ratios, overtime reduction, scope-of-practice changes), and whether labor partners are inside that conversation. Operators whose AI conversation lives only with IT are behind operators whose CNO and CHRO are in the same room as the CMIO.
Source: Chief Healthcare Executive
4. Market Signals
OpenAI Launches Healthcare Platform with Nine Flagship Health Systems
🔴 Major Product Launch | Score: 8.0 | View Article
Why It Matters OpenAI for Healthcare launched as a HIPAA-compliant enterprise platform with named flagship partners spanning academic medicine, integrated delivery, and specialty cancer. The partner list, not the product description, is the strategic message.
Key Details
- Vendor: OpenAI
- Named flagship partners: Stanford Medicine Children's, HCA Healthcare, Baylor Scott & White, Cedars-Sinai, AdventHealth, Memorial Sloan Kettering, Boston Children's, UCSF
- Same-week production proof point: Vanderbilt patient-facing OpenAI/Azure LLM deployment
- Adjacent context: Issue 7 (April 28) covered OpenAI's free clinician workspace; this is the enterprise productization
What This Signals The "model layer commoditizes" thesis is dead inside healthcare. Foundation model vendors will do enterprise sales, HIPAA compliance, and named-system co-development work to own the clinical workflow surface. Epic, Microsoft, AWS, and Oracle Health face direct competition inside the same procurement cycles.
My Read Pair the OpenAI launch with the same-week Vanderbilt production deployment, and the play becomes legible. OpenAI is not running an experiment. It is publicizing the platform in the same news cycle that a major AMC validates the architecture in production. That is coordinated, and it is the playbook every other foundation model vendor will copy. CMIOs need a position this quarter on whether their organization is a buyer, a partner, or a competitor in OpenAI's distribution play. Defaulting to "buyer" without a vendor selection framework locks systems into roadmaps they cannot influence.
Source: OpenAI
Bluesight Launches Prism: Agentic AI for Pharmacy Compliance
🔴 Major Product Launch | Score: 8.2 | View Article
Why It Matters Bluesight launched Prism, a generative AI platform purpose-built for drug diversion monitoring and pharmacy compliance workflows. Pharmacy compliance is a high-liability, low-automation, regulator-mandated category with sticky vendor contracts.
Key Details
- Vendor: Bluesight
- Product: Prism (generative AI platform for health systems)
- Use case: Drug diversion monitoring, pharmacy compliance workflows
- Stated security framework: Google Secure AI Framework referenced
- Category position: First major agentic AI in regulator-mandated pharmacy compliance
What This Signals Agentic AI is moving from front-office assistants and back-office RCM into compliance domains where switching costs are highest. Bluesight is positioning to be sticky.
My Read Pharmacy compliance is a regulator-mandated audit trail with DEA-level consequences for missed events; vendors that earn the trust of pharmacy compliance officers do not get easily displaced. Expect M&A interest from RCM consolidators looking for adjacent platform extensions. Health system pharmacy leadership should evaluate now, while procurement competition is moderate, not after a diversion incident creates emergency procurement conditions.
Source: Bluesight
AstraZeneca Licenses Owkin's Agentic AI for R&D Acceleration
🔴 Major Product Launch | Score: 7.2 | View Article
Why It Matters AstraZeneca licensed Owkin's agentic AI platform for federated R&D workflows. Pharma is now licensing, not partnering, not piloting, agentic AI as core R&D infrastructure.
Key Details
- Pharma sponsor: AstraZeneca
- AI vendor: Owkin
- Deal structure: Licensing agreement (not collaboration)
- Use case: Agentic AI for federated R&D workflows
- Adjacent pattern: Lilly-Insilico, Lilly-Profluent, Roche-PathAI all moved to licensing/acquisition terms in prior 30 days
What This Signals The pharma-AI corporate boundary continues to dissolve. Specialty AI vendors with credible biology output are commanding licensing-level commercial terms, better economics than research collaborations.
My Read Licensing implies repeatable deal terms, multiple competing buyers, and a different valuation profile than service contracts. For AI vendors, the structural read is that pharma R&D leadership is treating AI infrastructure as non-discretionary, which means the next round of competitive deal terms will be set by AstraZeneca, Lilly, and Roche, not by venture markups. AI biology vendors without licensing-grade IP and federated capability are about to be priced as services companies, not platforms.
Source: BusinessWire
5. Policy and Regulation
FDA Clears Bayesian Health's TREWS: First Continuous AI Sepsis Tool with Mortality Data
🔴 Policy / Regulation | Score: 8.5 (High Signal) | View Article
Why It Matters FDA cleared the first continuous AI sepsis early-warning system, backed by multi-site validation evidence showing earlier detection and approximately 18% reduction in in-hospital mortality. Clearance positions the product for NTAP reimbursement.
Key Details
- Vendor: Bayesian Health
- Academic anchor: Johns Hopkins University
- Clearance type: FDA 510(k)
- Achieved metric: ~18% reduction in in-hospital sepsis-related mortality (multi-site validation)
- Validation sites: Cleveland Clinic, MemorialCare, University of Rochester Medicine
- Reimbursement pathway: NTAP eligible
What This Signals Clinical AI now has a regulatory benchmark with mortality reduction attached. Every health system without a sepsis AI strategy now has a defensibility problem with their board governance. The next FDA clearances in cardiac decompensation, AKI, and ICU early-warning will follow the same evidence-to-clearance-to-reimbursement playbook.
My Read What separates this clearance from years of "AI early warning" press cycles is that the FDA evaluated mortality reduction, not just AUC or sensitivity scores. Every comparable vendor citing accuracy benchmarks now has to explain why their evidence base does not yet include mortality data. The named validation sites are not coincidental. They are the cohort that made clearance possible. Health systems that participate in pre-clearance validation cohorts get early access, named-partner credibility, and procurement leverage. Health systems that wait for clearance pay full price and inherit the procurement mandate.
Source: MedTech Dive
MACPAC Pushes CMS for AI Transparency in Medicaid Prior Authorization
🔴 Policy / Regulation | Score: 8.0 | View Article
Why It Matters MACPAC formally recommended that CMS impose transparency and human-oversight requirements on AI used by Medicaid plans for prior authorization, building on the WISeR backlash documented in Issue 7. Federal scrutiny of payer-side AI is hardening in the same week HHS is loosening provider-side AI rules.
Key Details
- Body: Medicaid and CHIP Payment and Access Commission (MACPAC)
- Target: CMS rulemaking on Medicaid prior authorization AI
- Recommendations: Transparency requirements, human-oversight mandates
- Companion context: WISeR Medicare prior auth pilot (Issue 5/7), state-level AI insurance laws (Issue 7)
- Provider tailwind: Denial management teams gain federal backing for transparency arguments
What This Signals Federal regulators are not coordinated on AI direction. HHS is proposing to lower the provider AI floor; MACPAC is pushing CMS to raise the payer AI floor. Operators inherit the integration problem.
My Read The political tailwind for contesting AI-driven Medicaid denials is real and worth resourcing. Health system denial management teams should treat MACPAC's recommendations as a near-term forecast of where Medicaid payer AI rules are heading, and build appeals infrastructure that takes advantage of the disclosure obligations before they are finalized. The window to recover historic AI-driven denials may open before it closes.
Source: Healthcare Dive
6. Funding Signals
Isomorphic Labs Secures $2.1B Series B: Largest AI Drug Discovery Round Ever
🔴 Funding Signal | Score: 8.2 | View Article
Why It Matters Alphabet, Thrive Capital, GV, Temasek, MGX, and the UK Sovereign AI Fund led Isomorphic's $2.1B Series B, the largest AI drug discovery round to date. Capital is deployed toward IsoDDE platform development and pipeline expansion.
Key Details
- Company: Isomorphic Labs (Alphabet-backed)
- Round size: $2.1 billion Series B
- Lead investors: Alphabet, Thrive Capital, GV, Temasek, MGX, UK Sovereign AI Fund
- Platform: IsoDDE (AlphaFold-derived drug design engine)
- Adjacent moves: Lilly-Insilico, Lilly-Profluent, AstraZeneca-Owkin, Roche-PathAI all reinforce platform-consolidation thesis
What This Signals AI drug discovery is consolidating around platform players with sovereign-fund-grade capital structures. The "many small bets" era is closing.
My Read The investor list is the moat. Sovereign funds and Alphabet do not exit on conventional venture timelines, which means Isomorphic has structural patience capital its competitors do not. Mid-cap AI biology vendors should stress-test their differentiation case before the next round, not during it. Pharma BD teams should expect Isomorphic terms to be reference comps in every comparable platform negotiation through 2026.
Source: Fierce Biotech
Anomaly Insights Raises $17M for AI-Powered Payer Intelligence
🔴 Funding Signal | Score: 7.5 | View Article
Why It Matters Anomaly Insights raised $17M led by Sound Ventures, Redesign Health, and RRE Ventures, with platform already deployed across 20+ health systems. Multi-system traction is the differentiator that justified the round.
Key Details
- Company: Anomaly Insights
- Round size: $17 million Series A
- Lead investors: Sound Ventures, Redesign Health, RRE Ventures
- Production deployment: 20+ health systems
- Category: Payer intelligence and revenue cycle AI
What This Signals Revenue cycle and payer-interaction AI is the next compounding category after ambient scribes. Multi-system traction is the moat that justifies Series A premiums in 2026.
My Read Expect a wave of payer-side AI vendors with comparable multi-system traction claims through 2026. Revenue integrity leaders should evaluate now, while procurement competition is moderate and the category leader is not yet established. The strategic question is whether to anchor on a standalone payer intelligence vendor or wait for EHR-native equivalents, and the 20+ system reference is the answer for buyers who cannot wait.
Source: MedCity News
7. Research Breakthroughs
JAMA: LLM-Based Preoperative Communications Reduce Patient Anxiety and Clinician Workload (RCT)
🔴 Research Breakthrough | Score: 8.2 | View Article
Why It Matters A randomized Phase II trial documented that LLM-generated preoperative communications significantly reduced patient anxiety scores and clinician documentation workload simultaneously. Peer-reviewed, randomized, with both patient experience and workload endpoints.
Key Details
- Study design: Randomized Phase II clinical trial
- Intervention: LLM-generated preoperative patient communications
- Patient outcome: Reduced patient anxiety scores (statistically significant)
- Clinician outcome: Reduced documentation workload
- Publication venue: Peer-reviewed (The ASCO Post coverage)
What This Signals Patient-experience AI use cases are now publishable in peer-reviewed venues with hard outcome endpoints. Vendors with only satisfaction-score data face rising procurement scrutiny.
My Read The dual-endpoint design is the structural detail. Most clinical AI studies report either workload reduction or patient experience improvement, not both. Demonstrating both simultaneously closes the procurement objection that workload AI sacrifices patient experience. Vendors selling patient-facing or preoperative AI should plan to publish comparable dual-endpoint evidence inside 12 months, or expect to lose RFPs on evidence grounds.
Source: The ASCO Post
Providence + Microsoft Validate TRIALSCOPE for AI-Driven Cancer Clinical Trials
🔴 Research Breakthrough | Score: 8.2 | View Article
Why It Matters Providence and Microsoft validated TRIALSCOPE, an AI platform constructing simulated control arms from real-world EHR data, accelerating oncology trial design. Two halves of the trial bottleneck (recruitment and controls) got AI attacks in the same week (Cleveland Clinic Synapsis on recruitment, Providence TRIALSCOPE on controls).
Key Details
- Organizations: Providence, Microsoft
- Platform: TRIALSCOPE
- Capability: Synthetic control arms from real-world EHR data
- Use case: Cancer clinical trial acceleration
- Adjacent context: Cleveland Clinic Synapsis trial recruitment (same week)
What This Signals Microsoft's healthcare-specific AI investments are producing regulator-credible outputs. The Providence-Microsoft alliance is now a credible counterweight to the Epic-centric integration narrative.
My Read Pharma trial sponsors will start asking site partners about real-world evidence and synthetic control capability in addition to recruitment velocity. Research operations leaders without a real-world evidence capability are about to be deprioritized in pharma site selection. The strategic implication for AMC competitive positioning: the next 18 months of trial-site competitive advantage will be defined by AI infrastructure for recruitment and synthetic controls, not just patient volume.
Source: Chief Healthcare Executive
8. Trend to Watch: The Federal Floor Drops While State, Payer, and Clinical Floors Rise
This week's federal signals do not point in a single direction. HHS proposed easing AI transparency requirements. The FDA cleared a continuous AI sepsis tool with a mortality endpoint, demanding evidence to defend. MACPAC formally pushed CMS toward tighter prior authorization AI oversight. Three agencies, three different directions, in the same five-day window.
The implication for health system AI governance is operational. The HTI-1 transparency floor that vendor risk programs were built around is becoming negotiable. Below it, state AGs (Pennsylvania v. Character.AI, ongoing), state insurance commissioners, and payer audit programs are layering rules that bypass federal preemption. Above it, the FDA's clinical AI clearance bar is rising, anchored by mortality endpoints and named-system validation cohorts. The compliance burden is increasing in net, not decreasing, and operators inherit the integration problem of governing AI against a fragmented compliance map.
The right posture this quarter: assume the federal floor is moving down, assume state and payer floors are moving up, and design AI procurement, governance, and disclosure infrastructure to the higher of the two, regardless of what HHS rulemaking ultimately produces.
9. Signal Scoreboard: Top 10
- Proposed HHS Rules Easing AI Health IT Safeguards | 8.5 | PolicyFederal transparency floor becomes negotiable
- FDA Clears Bayesian Health Continuous AI Sepsis Tool | 8.5 | Policy/ResearchFirst continuous clinical AI with 18% mortality endpoint
- Cleveland Clinic Synapsis 7x Trial Recruitment | 8.5 | DeploymentPeer-reviewed operational lift at flagship AMC
- Stanford 60% Utilization on Enterprise Admin AI | 8.2 | DeploymentAdmin AI utilization benchmark at flagship
- Isomorphic Labs $2.1B Series B | 8.2 | FundingLargest AI drug discovery round ever
- Bluesight Prism Pharmacy Compliance | 8.2 | ProductAgentic AI enters high-liability compliance
- JAMA RCT: LLM Preop Communications | 8.2 | ResearchDual-endpoint clinical AI RCT
- Providence + Microsoft TRIALSCOPE | 8.2 | ResearchSynthetic control arms move to production
- MACPAC AI Prior Auth Oversight | 8.0 | PolicyFederal scrutiny on payer-side AI hardens
- OpenAI Healthcare Platform Launch | 8.0 | ProductFoundation model direct flagship distribution
10. Noise of the Week
Hippocratic AI Announces Executive Appointments
🟡 Funding Signal | Score: 3.1 | View Article
Why It Matters Hippocratic AI is one of the most-watched agentic healthcare AI vendors; senior leadership additions typically precede scale milestones.
Key Details
- Vendor: Hippocratic AI
- Announcement: Senior executive appointments
- Named deployments: None
- Live outcomes: None
- Prior coverage: Polaris 5.0 announcement also classified as noise in Issue 8 (May 1)
What This Signals Two consecutive press cycles without a deployment proof point. The pattern is the signal.
My Read Vendor announcements of leadership additions, product version bumps, and benchmark claims without named customers and measurable outcomes are not market signal. Procurement teams evaluating Hippocratic AI should ask for named deploying health systems, peer-reviewed validation, and production-volume outcome data. Until those are public, this is positioning theater.
Source: PR Newswire
Forbes: Healthcare AI Adoption "Quiet Revolution"
🟡 Commentary | Score: 3.2 | View Article
Why It Matters Forbes byline, sweeping framing on healthcare AI adoption attitudes.
Key Details
- Publication: Forbes (Tech Council)
- Subject: Healthcare AI adoption commentary
- Named organizations: None
- Live workflows: None
- Measurable outcomes: None
What This Signals Trend commentary without primary evidence.
My Read Industry attitude pieces without named organizations or measurable outcomes provide no decision-grade information. Reference for sentiment, not strategy.
Source: Forbes
11. Executive Takeaway
The federal accountability stack is being disassembled and reassembled in the same week, and the reassembly is happening at higher altitudes than the original floor. State Attorney Generals, payer audit programs, and FDA clinical AI clearance evidence requirements are filling the space HHS is vacating. Govern your AI portfolio against the highest applicable floor, not the federal one. Add HTI-1-level transparency obligations to vendor contracts regardless of HHS rulemaking, build sepsis AI procurement around the new Bayesian Health benchmark, and treat MACPAC's recommendations as a near-term forecast of Medicaid payer AI rules. Initiatives that cannot survive the higher floor are not strategic assets. They are exposure.
Healthcare AI Signal is a high-signal briefing on the developments actually shaping AI in healthcare. healthcaresignal.ai